Tuesday: Fitness Do’s (Sagittal Plane Restoration)
Why start with movement correction in the sagittal plane?
The sagittal plane can refer to both forward active movements (running, crawling, lunging) and more fixed stationary movements like squatting and tilting of the pelvis (forward or back).
However, running, for example, also involves a side to side movement (in the frontal plane) as the weight shifts from one leg to another and rotational (transverse plane) movement of the pelvis rotating towards the fixed femur.
So, when we discuss running as a sagittal plane movement we are implying a forward direction or movement of an arm or leg moving forward or back.
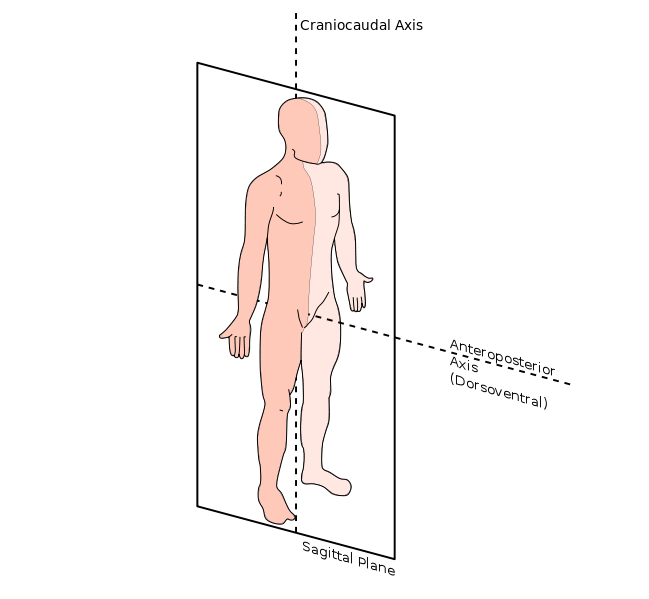
The sagittal plane divides the body into two halves a left and a right side. So, the contralateral movement of the opposite arm and leg propels the body forward in the sagittal plane – even though this involves a transverse plane (rotational) component.
Ribs have to rotate for arms to swing.
This discussion will look at hip flexion and hip extension (movement of the extremities) but will focus on the stabilizing center of gravity in the middle (thoraco-pelvic canister) that creates a fixed point for movement of the extremities (arms and legs).
I will be discussing four treatment approaches that I utilize to restore movement in the sagittal plane and why this plane of motion, in particular, is so important (from different perspectives).
This was meant to be a shorter Instagram post, but I have a book in the works and this blog has allowed me to clarify some thoughts on the subject. I hope you ENJOY!
#1: Dynamic Neuromuscular Stabilization (A Developmental Perspective)
The Prague School of Rehabilitation has outlined normal, expected milestones for the developing child. The first of which is the three month old position of the child on their back or stomach. These are referred to as 3M Supine and 3M Prone.

The 3 Month position is an important milestone because it is when the child first begins to integrate the diaphragm with the abdominal all and pelvic floor to establish sagittal stability of the trunk and pelvis. Evan Oscar uses the term the “Thoraco-pelvic canister.” In sub-system language, this is referred to as the Intrinsic Stabilizing Subsystem (ISS).
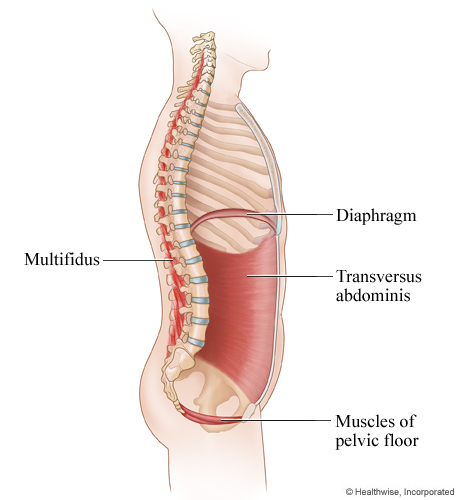
DNS practitioners use developmental positions to reinforce proper mechanics of stabilization. One of their major contributions to the understanding of movement is their discussion of ‘fixed points.’ Distal movement (of the extremities) requires proximal stabilization of the trunk.
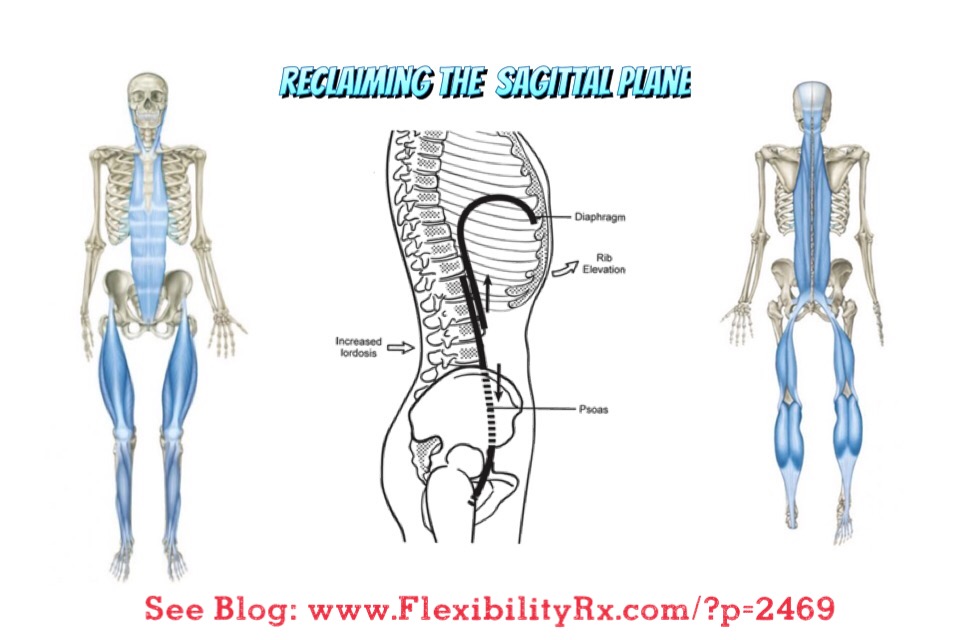
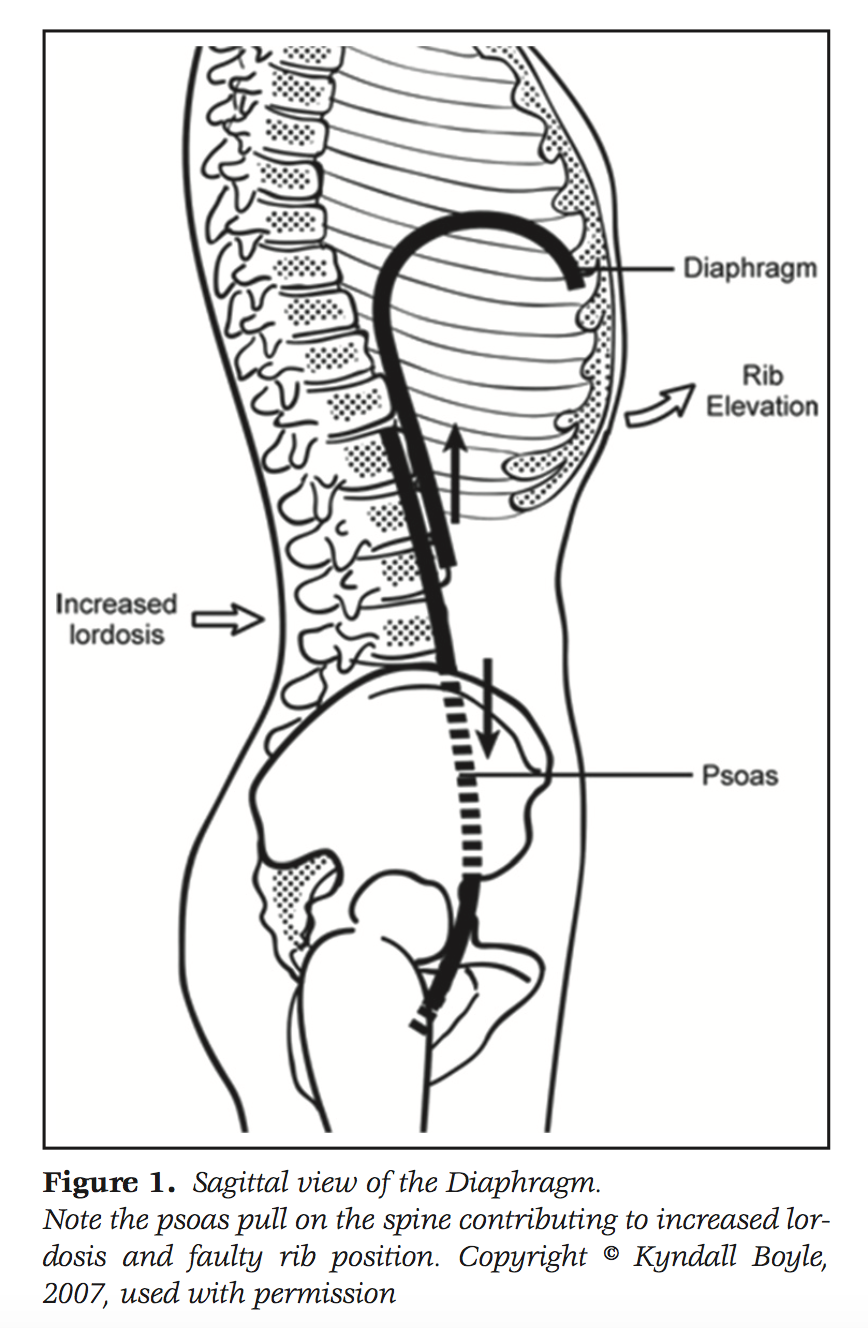
Flexion and extension movements of the arms and legs require core stability as an anchor point for movement. The psoas when acting as a flexor of the hip needs to have a stable spine to anchor from. The following DNS image shows the interplay of this intrinsic stability during flexion of the hip and shoulder in human locomotion. When the thoraco-pelvic canister does not act as a punctum fixum – walking and sagittal plane movements will be compromised and replaced with a compensatory stabilization strategy.
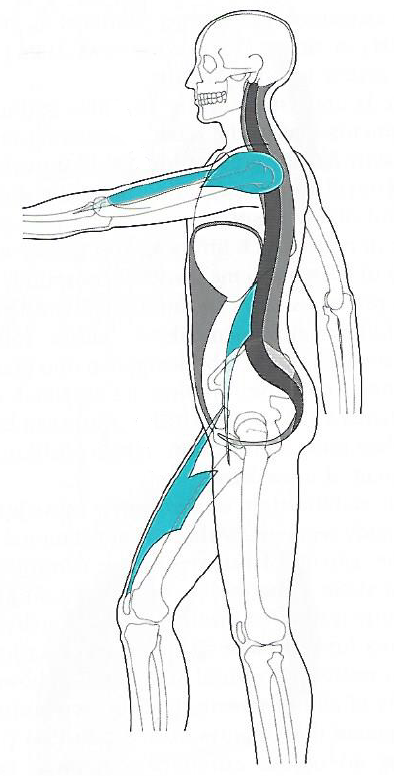
Image taken from book, “Recognizing and Treating Breathing Disorders”
When someone does not have proper alignment, they will commonly default to a compensatory pattern which DNS refers to as the Extension Compression Stabilizing Strategy (ECSS).
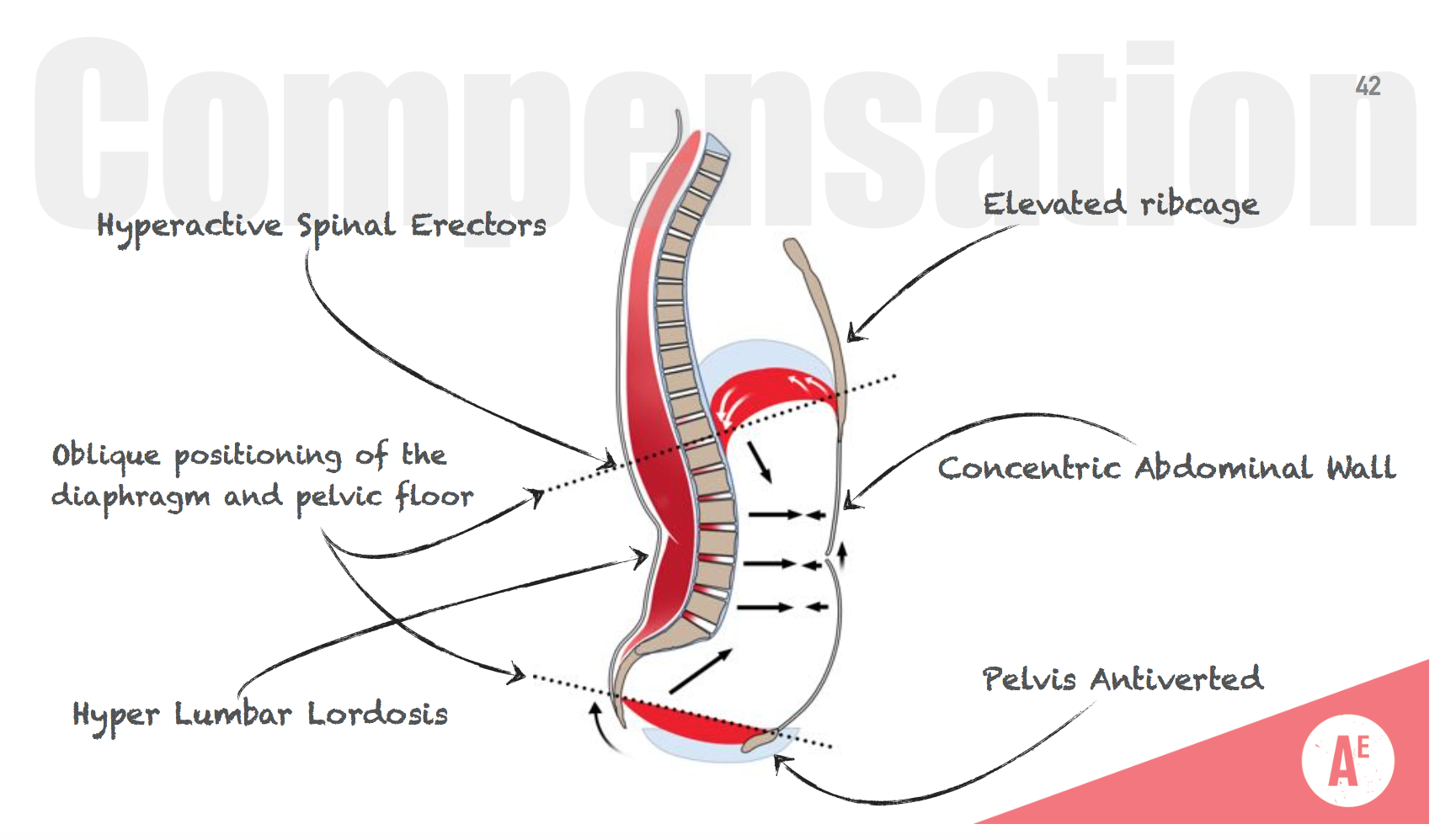
image courtesy of DNS Instructor Richard Ulm – Athlete Enhancement
Vladimir Janda referred to this as the ‘Lower Crossed Syndrome.’ The Postural Restoration Institute refers to the muscles that hold this pattern in place as the Posterior Exterior Chain (PEC). In this case the Latissimus Dorsum, Quadratus Lumborum, Posterior Intercostals, Serratus Posterior, and Iliocostalis Lumborum are all overactive in an individual with a bilateral ECSS strategy.
#2: Structural Integration & The Anatomy Trains
Tom Myers has provided another theory of movement and organization of the body. His concept consists of three cardinal longitudinal lines of myofascial that span the body from the ball of the foot to the neck/head. These three lines are referred to as the superficial front line, the superficial back line, and the lateral line (s).
“If the front and back lines are the north and south of the body, then the two lateral lines are east and west. For this reason, we all these three lines taken together the cardinal lines, as they define the cardinal points of stability in our human compass – front, back, right, and left.” – Tom Myers
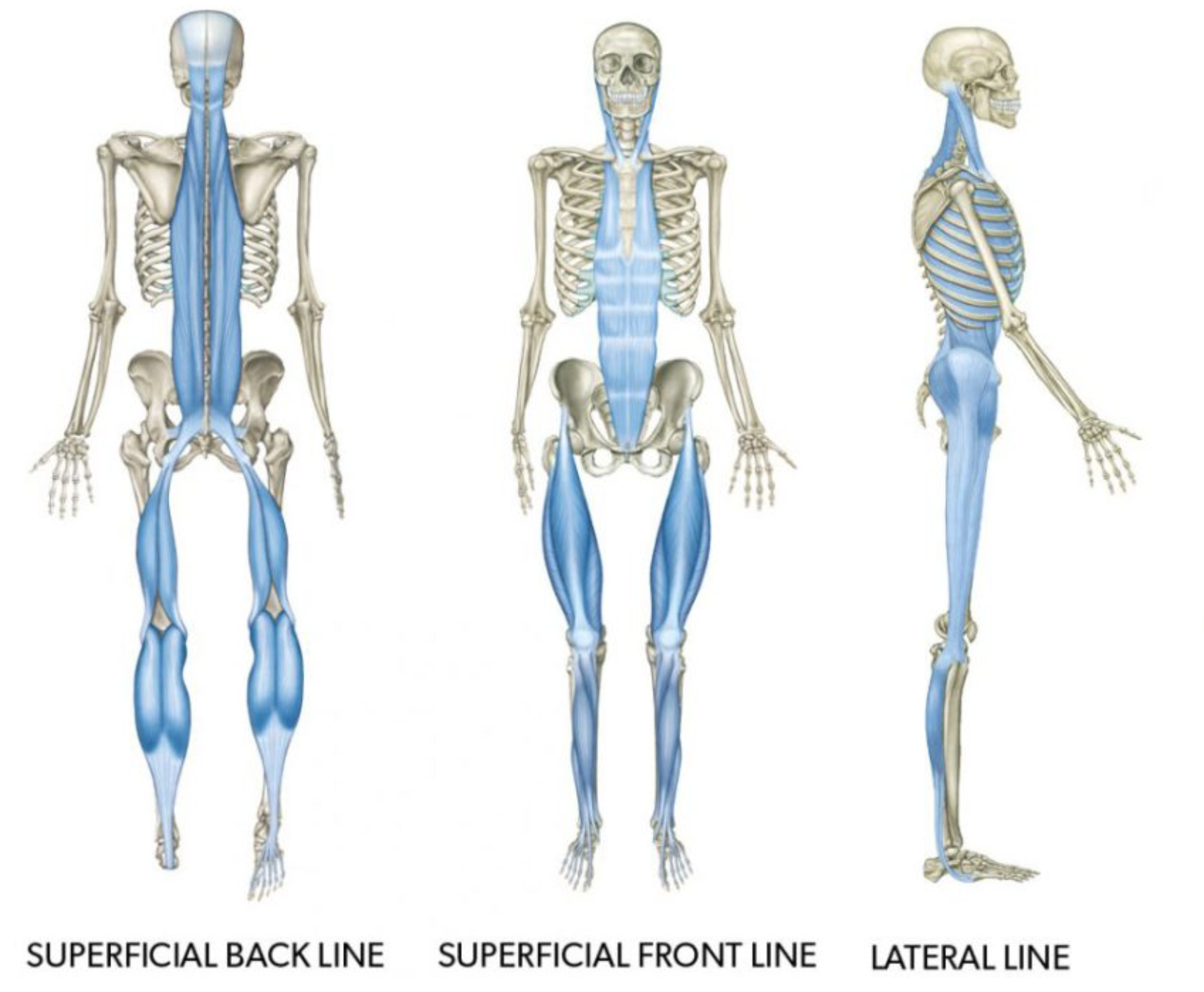
This discussion will limit itself to the SFL and SBL. While the lateral line does provide stability – balancing the front and back, it’s influence is once seen in postural compensations the frontal plane.
Going back to the 3M Prone position the baby on their stomach lifting their head begins to contract the SBL.
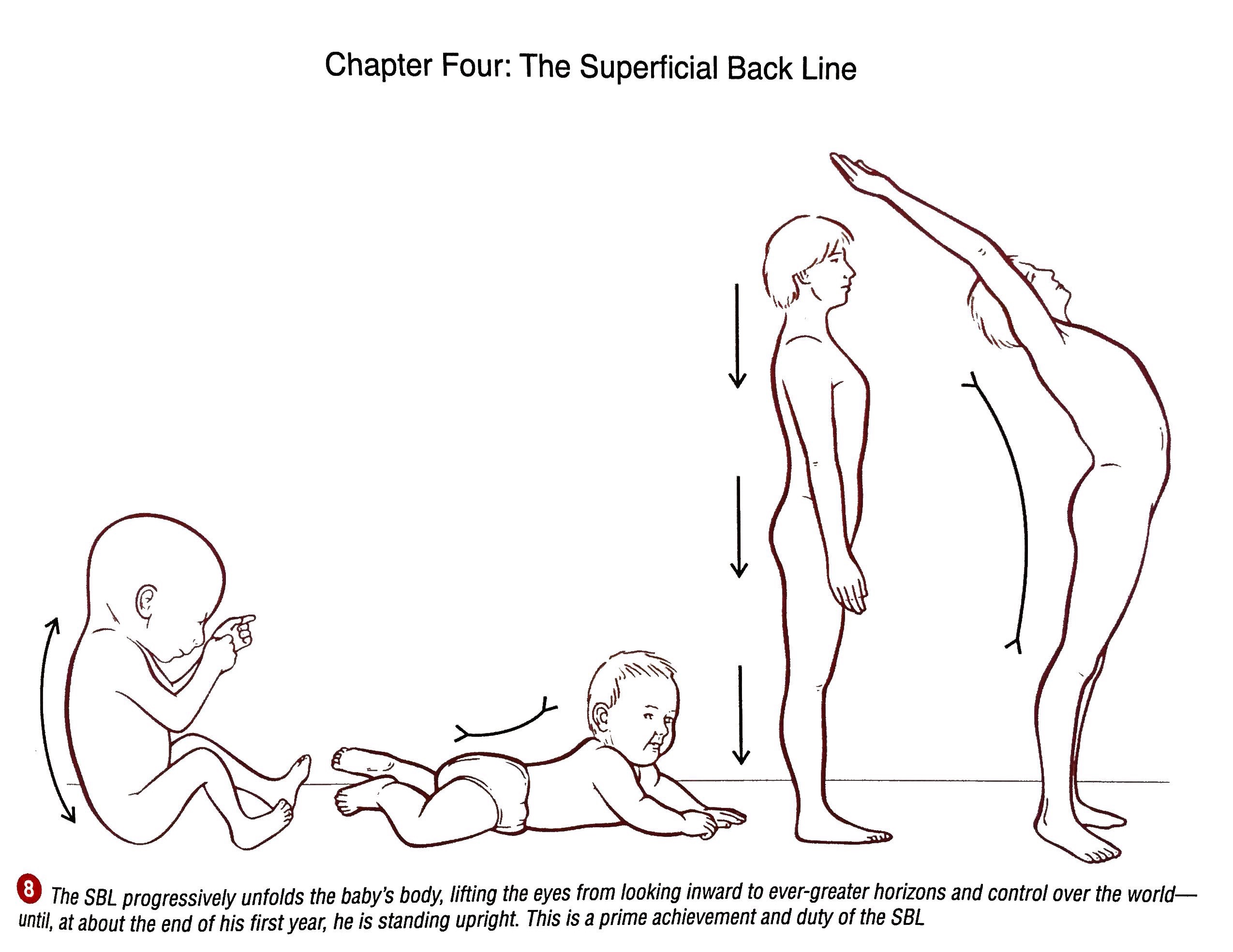
“For our precarious human standing to work, the long and singular primary C-curve of the fetal spine we see at the left side in Image 8 has to turn into a series of waves we call primary and secondary curves. As a baby lifts its head, the muscles in the back of the neck strengthen enough to change the shape of the discs and allow the neck to bend from concave forward to concave backward – in other words, into a secondary curve.”
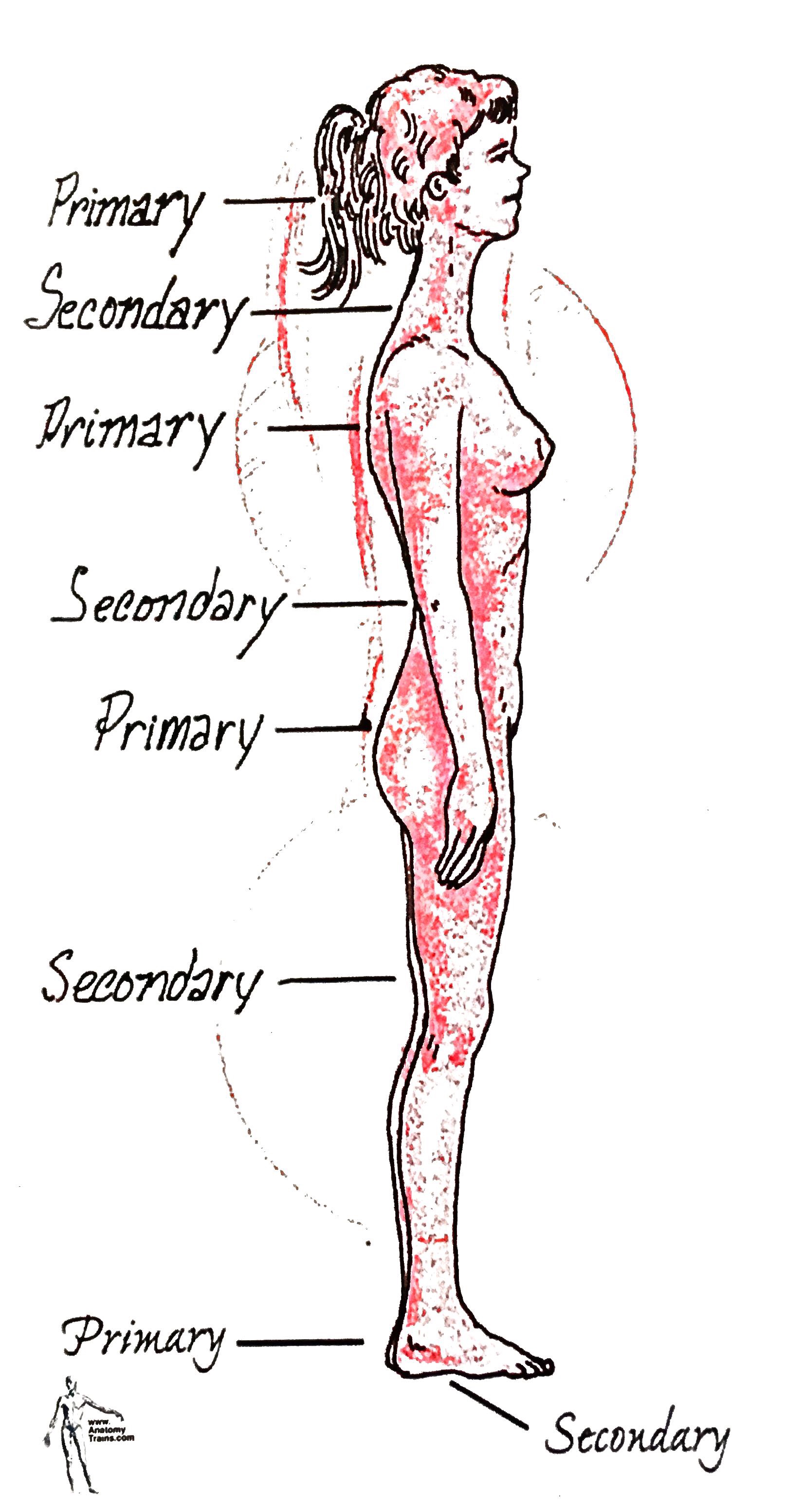
He explains that the spine has two original primary curves (thoracic, sacral) held in place by bony support and two secondary curves (cervical, lumbar) held in place by the balance of the surrounding myofascial). He expands upon the concept of primary and secondary curves in the picture above.
Structural Integration sessions aim to restore balance in the myofascial that often turn secondary curves (like the lumbar spine and knees) into primary curves. In other words, an ECSS strategy compresses the lumbar spine turning it into a primary curve – both functionally and physically as tissue change over time influences its shape.
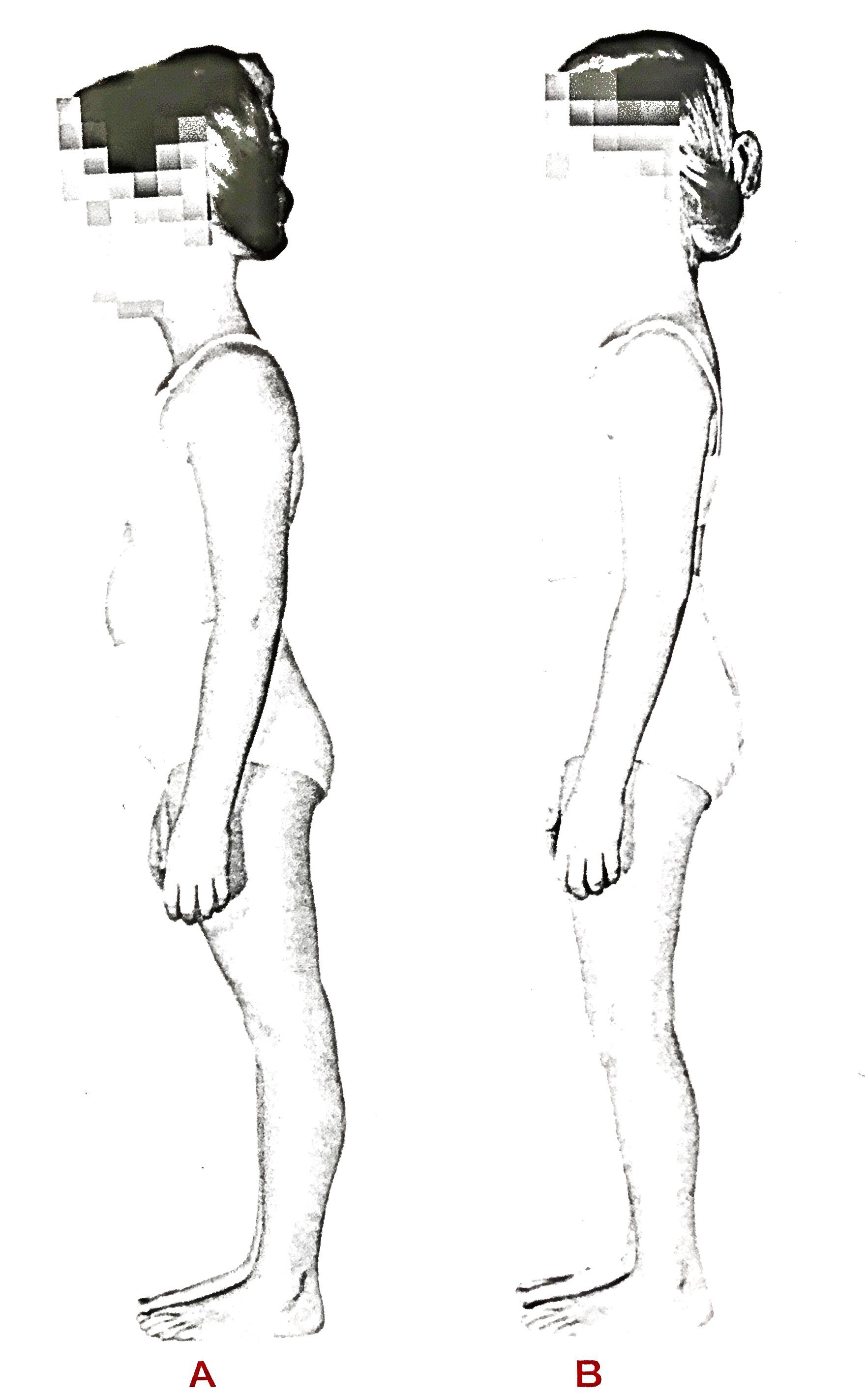
Individuals with chronic low back pain need to soften their knees in order to influence change in the lumbars and cervicals (see photo of girl bellow). This recognition of primary and secondary curves in the sagittal plane affords a global strategy of treatment – as opposed to a manipulation of a single vertebrae, treatment at a single joint, or focus on one muscle.
#3: Postural Restoration Institute (PRI)
So far, we have been viewing the body from a bilateral perspective (assuming that Tom Myers left and right portions of the SFL or left and right SBL trains are holding the same pattern in place). When we use the terms PEC, Extension Compression Stabilizing Strategy, Lower Crossed Syndrome we are generally referring to a bilateral pattern.
All four of the treatment modalities here use appropriate assessment to consider the left and right sides of the body that influence the sagittal plane.
However, PRI begins their treatment strategy with a discussion of predictable asymmetry. Not asymmetry that life has created but asymmetry that is governed from an ingrained respiratory, neurological, and biomechanical drive.
For the sake of this discussion I will focus on the relevance of having an asymmetrical diaphragm and the respiratory mechanics of the right diaphragm on the sagittal plane.
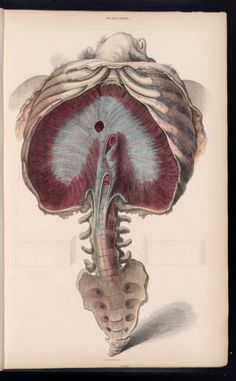
The Postural Restoration Institute points out that the RIGHT hemi-diaphragm
Has a larger diameter
Thicker central tendon
Larger central tendon
Higher central dome
Is better able to maintain its dome shape (supported by the liver)
Has more crura fibers and fascia (which influence the spine)
Has crura that attach lower 1 ½ levels lower on the lumbar spine
Has better abdominal eccentric opposition (more toned R abs)
Is concentrically effective for respiration
This results in a more flared left ribcage that is in need of better opposition from the abdominals (internal obliques and transverse abdominis) to concentrically bring the ribcage back down via an exhalation.

This sagittal plane restoration is referred to as obtaining a ZOA (Zone of Apposition).
This obtainment of a Left ZOA requires left hamstring and abdominal integration.

PRI practitioner Ryan Dobbeck: https://www.instagram.com/dobbecktraining/
An athlete then has to eccentrically maintain this ZOA so that they can rotate through their trunk and stabilize their pelvis in the transverse plane while walking – without flaring their left ribcage. For arms to swing ribs need to rotate. The transverse plane momentum during gait is dependent on preservation of a sagittal plane.
“Our asymmetrical pattern of breathing regulates the position and function of three keystone type bones positioned centrally along the midline of our body called the sternum, sacrum, and sphenoid. Our breathing pattern further serves to stabilize each of these bones in a non-neutral position from which they are attempting to function while the structures around these bones are in an asymmetrical position.” (PRI Integration for Fitness Manual)
The PRI exercise of Ryan above is influencing his LEFT superficial back line (hamstring activation) and his RIGHT superficial front line (quadriceps activation).
The right diaphragm’s influence on the pelvis often results in anterior pelvic tilt on the LEFT and posterior pelvic tilt on the RIGHT. Here he is rebalancing his pelvis in the sagittal plane.
This brings us to muscle testing…
#4: Manual Muscle Testing (Neurokinetic Therapy)
Muscle testing provides different entry points into the nervous system including assessment of vision, breathing, individual muscle functions, and global stabilization patterns.
A series of tests, in particular, that I like to use are global perturbation tests. NKT Instructor Perry Nickelston (Stop Chasing Pain) does an amazing job in his own workshops of examining these planes of motion.
If we look back at the Anatomy Trains we appreciate the role that they play in upright posture. One way of assessing global stabilization patterns are standing perturbation tests. Basically, the examiner applies force through one of Tom Myers cardinal planes – pushing the person back, forward, or laterally on each side. This is a great entry point (globally) for more specific local testing.
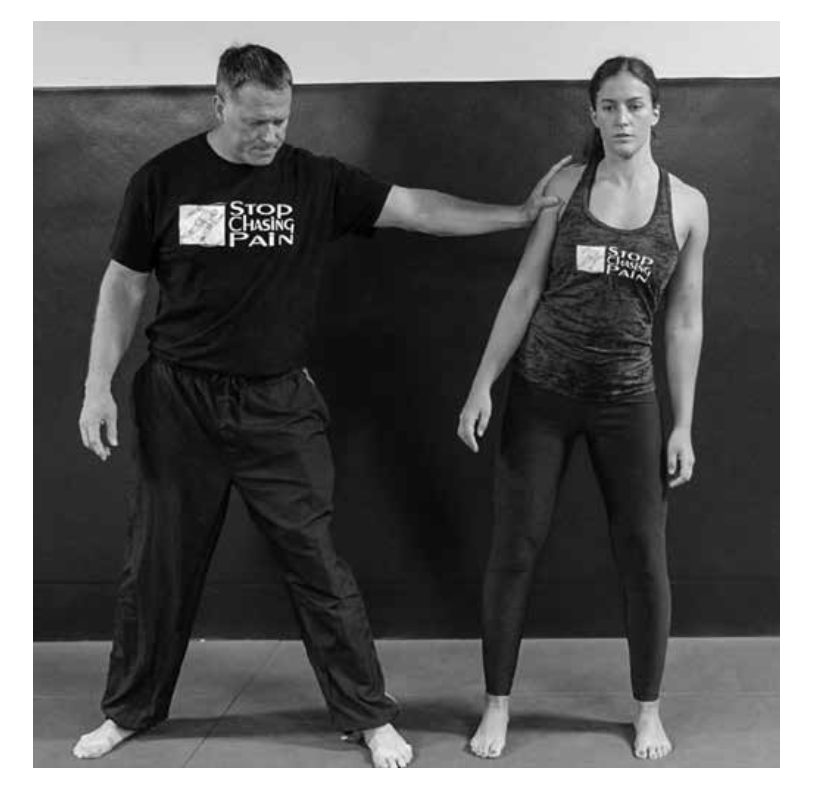
The picture above shows a perturbation test for the frontal plane (lateral pressure). The sagittal plane tests would involve a forward or backward pressure.
One way of assessing these planes of motion on your own is the Bunkie Tests. The image below is one way of assessing the sagittal plane.
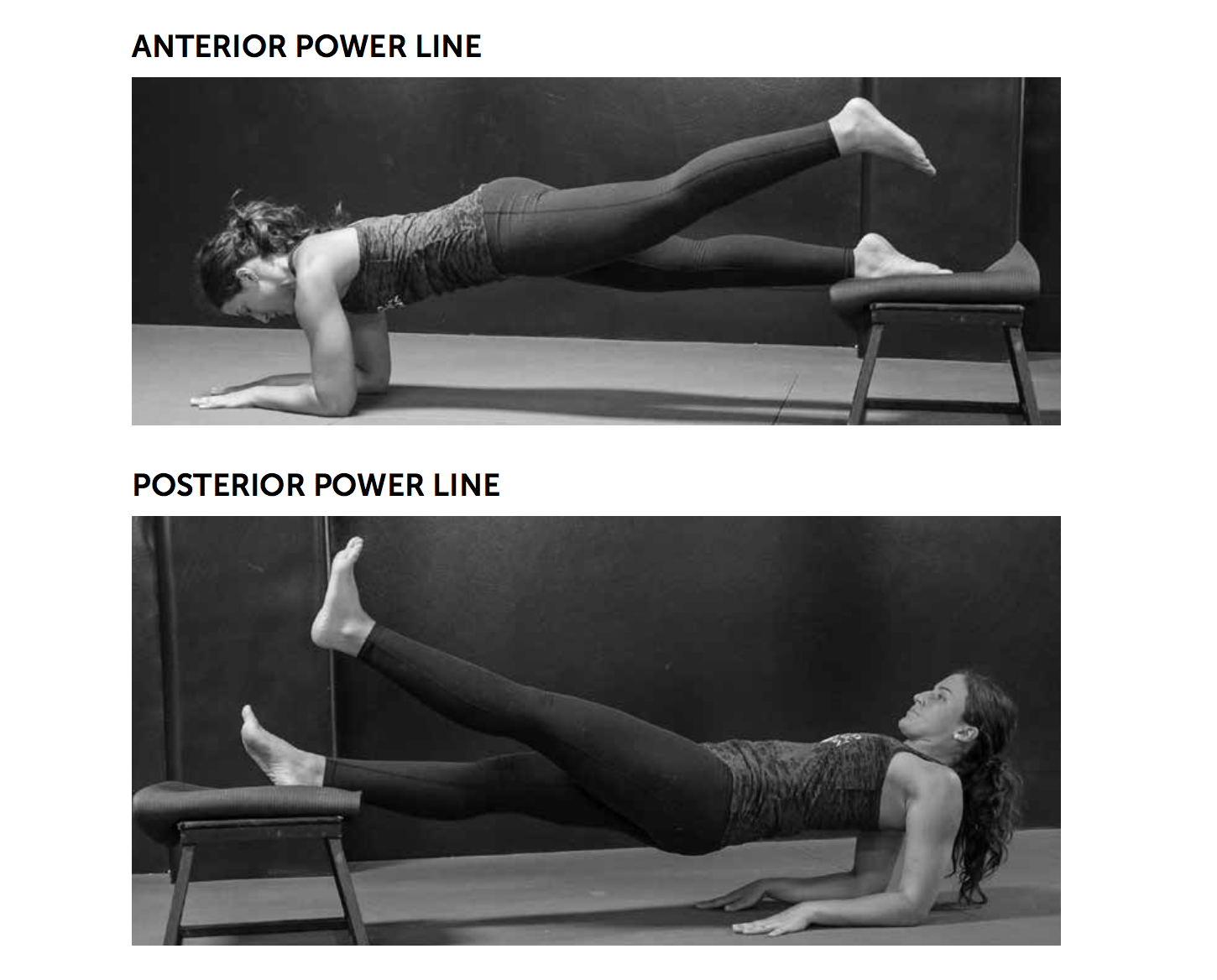
Image taken from Perry Nickelston’s Course Manual – www.stopchasingpain.com
I think sometimes trainers and manual therapists get confused when looking at the Anatomy Trains. This comes from thinking of one whole line always functioning against another line (front and back). Parts of the front line may be overactive making up for parts of the back line. Muscle testing allows someone to test their client in a way so that they can understand what individual muscle group needs soft tissue work or retraining. This is also a way of separating out the left and right sides of the superficial front or superficial back line.
David Weinstock (NKT) has done an amazing job of synthesizing muscle testing and making muscle testing learnable, relevant, and integrative.
Self-Assessment & Treatment of the Sagittal Plane
I will save more in-depth assessments and treatment options for another post. This assessment template is something I utilize in my FlexibilityRx workshops. However, here are three considerations when looking at the sagittal plane.
#1: How is My Pelvis Positioned on One or Both Sides?
Meaning bilateral anterior tilt or left anterior/right posterior for example. This can be assessed by looking at hip extension range of motion in quadruped. Does the lumbar spine compensate for lack of hip flexion?
#2: Do I Have Ribcage Flare on One or Both Sides?
This can be addressed by including one or two positional breathing drills pre-workout. To combat left ribcage flare include an exercise that integrates the left hamstring with the left ab wall.
#3: Use the Bunkie Tests to Assess Long Lever Influence on the Sagittal Plane
There are 5 total involving the left and right side so 10 tests. Each of the Bunkie Tests require the Intrinsic Stabilizing Subsystem to stabilize the trunk. You should be able to hold each of the Bunkie tests for 30 seconds.
– Kevin J. Kula, “The Flexibility Coach”
Leave A Reply (No comments so far)
You must be logged in to post a comment.
No comments yet