
Thursday Fitness Don’ts: Hamstring Over-Stretching

Hamstring Laxity & TMJ (The Connection)
Jaw pain is one of the seemingly hardest conditions to treat. Facial tension, jaw clicking/popping, grinding of the teeth – these are chronic conditions oftentimes chiropractors, physical therapists, and dentists struggle to find solutions for. Other than stress what factors are literally causing many individuals to chew through their mouth guards?
Signs and Symptoms of TMJ Disorders
Pain or tenderness of the jaw and facial muscles
Difficulty chewing or pain while chewing
Clicking or popping sounds in the jaw when chewing
Headaches
Aching pain in and around the ear
Ringing in the ears
Dizziness
Before discussing the correlation, I found between hamstring laxity and TMJ in women (and what led me to examine that relationship) here are a few things.
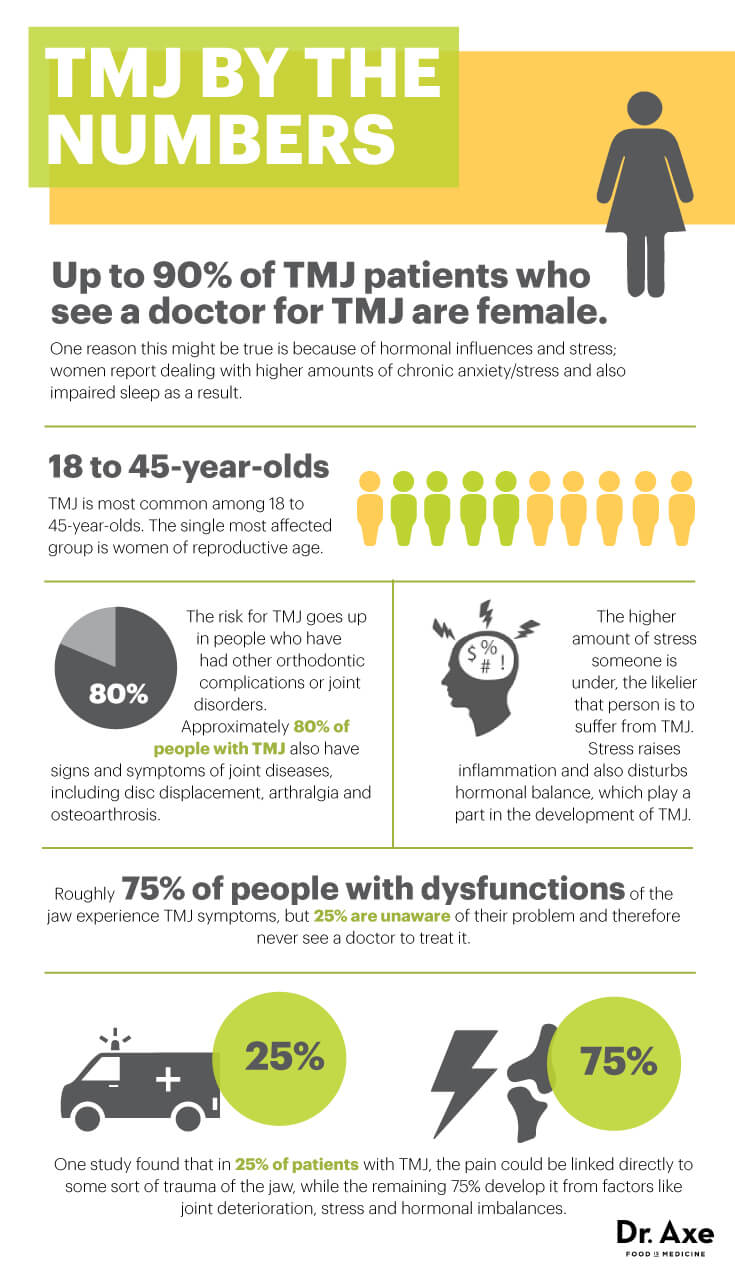
TMJ is a persistent condition with many provoking factors. The abbreviation TMJ (Temporal Mandibular Joint) generally refers to jaw pain. Personally, I have encountered more women than men with TMJ disorder (as indicated by intake forms). I am unsure of the reliability of these statistics but Dr. Axe reported that there are over 10 million people in the U.S. that suffer from TMJ. His numbers show that ninety percent of TMJ patients who see a doctor for TMJ are female.
One of the biggest discussions concerning women suffering from TMJ is the role hormones may play. TMJ is most common among 18 to 45-year-old women – the single most affected group is women of reproductive age. Increased hip flexibility is a byproduct of female hormones that help to prepare women for pregnancy.
Men have a greater collagen density than women which makes women more prone to laxity/instability. There are also more women that are drawn to yoga than men (which can involve a lot of hamstring stretching). In terms of athletics Mike Reinold points out in his book, “The Athlete’s Shoulder” that:
“There are unique concerns when treating the female athlete. Many male athletes are regular participants in a weight-training program. Large muscle groups such as the latissimus dorsi, pectoralis major, and biceps brachii are well developed and sometimes do not need to be specifically addressed in rehabilitation; the stabilizing rotator cuff and scapular musculature are the focal points during treatment. Conversely, fewer female athletes participate in weight-training programs. Large muscle groups that serve as prime movers might need to be addressed to assist with appropriate sport biomechanics for this population.” – Mike Reinold
The Beighton tests screen for laxity. I regularly use these with young gymnasts and dancers – in addition to seeing how well they use muscular effort to stabilize rather than relying solely on their joints and ligaments for stability.
“We all have a certain degree of laxity. A high Beighton score does not indicate that they have a syndrome or problem, it just helps determine where they sit in the laxity spectrum. A high amount of laxity does not necessarily mean you have instability. Stability is a combination of the function of your static and dynamic stabilizing systems. Instability is when you have an issue with either (or both) of the static and dynamic stabilizers. Functional stability is the ability to dynamically stabilize a joint during functional activities to allow proper control and movement.” – Mike Reinold
Estrogen, the female hormone, dramatically inhibits fibroblasts. These fibroblasts are what make the collagen that makes up the ligaments and tendons, which are injured during sports or other chronic pain injuries. The more estrogen some women have, the more inhibition may occur. There are estrogen receptors on the anterior and posterior cruciate ligaments (more commonly injured in women), Achilles tendon, and in skeletal muscle – http://lermagazine.com/article/influence-of-estrogen-on-the-plantar-fascia.
This is not an article about hormones or ligament laxity. This is just a primer on gender differences that may explain why women who are more prone to HAMSTRING laxity also are more prone to TMJ.
It is this correlation (that I have examined) that I believe provides an interesting explanation for a higher percentage of TMJ in women.
This Article Will Examine:
#1: The relationship of pelvic instability (anterior pelvic tilt) and cranial bone position.
#2: The reason why I would look for a relationship between hamstring laxity and TMJ.
#3: How I screened for a correlation of hamstring laxity and TMJ.
#4: My findings and why this often-overlooked connection is so important.
#5: How you can self-treat TMJ (at least the most relevant global components).
I Hope you enjoy! Please share this article.
#1: The Relationship Between Anterior Pelvic Tilt & Cranial Bone Position
Dr. Rothbart, a podiatrist published a study that examined the link between altered cranial bone positioning and abnormal foot motion entitled, “Vertical Facial Dimensions Linked to Abnormal Foot Motion.”
https://www.researchgate.net/publication/5362066_Vertical_Facial_Dimensions_Linked_to_Abnormal_Foot_Motion
Before we look into his findings here is a brief look at factors that influence the structure and position of bones…
Factors that Influence Bone Structure and Position
An individual that has adaptive changes in cranial bone positioning oftentimes exhibits an altered facial structure. This can be seen on an x-ray where the jaw actually changes it’s shape over time. This is commonly seen as a pointed chin. This type of individual will over-recruit their digastrics and scalene muscles. The loss of a normal cervical curve here is correlated with hyperactivity of the muscles of the neck and jaw.
Another bony adaptation that can be seen via x ray is bone spurs on the foot. This is often the result of altered load bearing and which causes the bone to thicken over time.

Going back to the jaw, dentist Weston A. Price noticed that malnutrition has the ability to change facial structure across generations. Individuals with an underdeveloped maxilla will have a narrower face and restricted airway. The abandonment of a Paleo type diet that includes a lot of chewing of raw foods will not develop the jaw and results in a narrower face. For a comparison take a look at the well developed jaws and facial features of Robert Redford or Marilyn Monroe.
“When children or adults are not breathing properly they tend to develop dark patches and bags under their eyes. This is due to lack of adequate circulation as well as venous blood pooling in these areas. Also mouth breathers in profile tend to have very weak chins and elongated faces. Typically, these individuals will suffer from chronic sinusitis or sinus infections, colds, respiratory problems and lung-related issues. Typically, children with bags under their eyes have short attention spans because they do not have good circulation and oxygenation of the head and can tire easily. They are literally suffocating.” – Weston A. Price Foundation
I discussed this in my book review of, “GASP: Airway Health – The Hidden Path to Wellness.”
While nutrition will impact bone development – movement (alignment, posture, etc) influences bone position. Structural Integrators (a type of bodywork) often include intra-nasal work at some point in their sessions with patients to open up the nasal passage and re-align the cranial bones.

What this means is that certain facial characteristics are alterable (via bone position) whereas some are not (due to the physical structure of the bones).
There is a difference between bone growth (structure) and bone position (dynamic alignment). Over time in conditions like spinal stenosis change the structure of the bone. In the case of stenosis there is a narrowing of the spinal canal due to abnormal bone growth*.
*This is commonly due to poor core stabilization and resultant compression of the lumbar discs as a compensatory stabilization strategy. I discussed this in my post, “Reclaiming the Sagittal Plane.”
The interplay between structure, form, and function is nicely explained by the following equation…
“Movement becomes habit, which becomes posture, which becomes structure.” – Tom Myers
Osteopaths have certain categories for predictable types of cranial strain patterns.
The Postural Restoration Institute talks about two very common cranial strain patterns: A Right Torsion and a Left Sidebend.
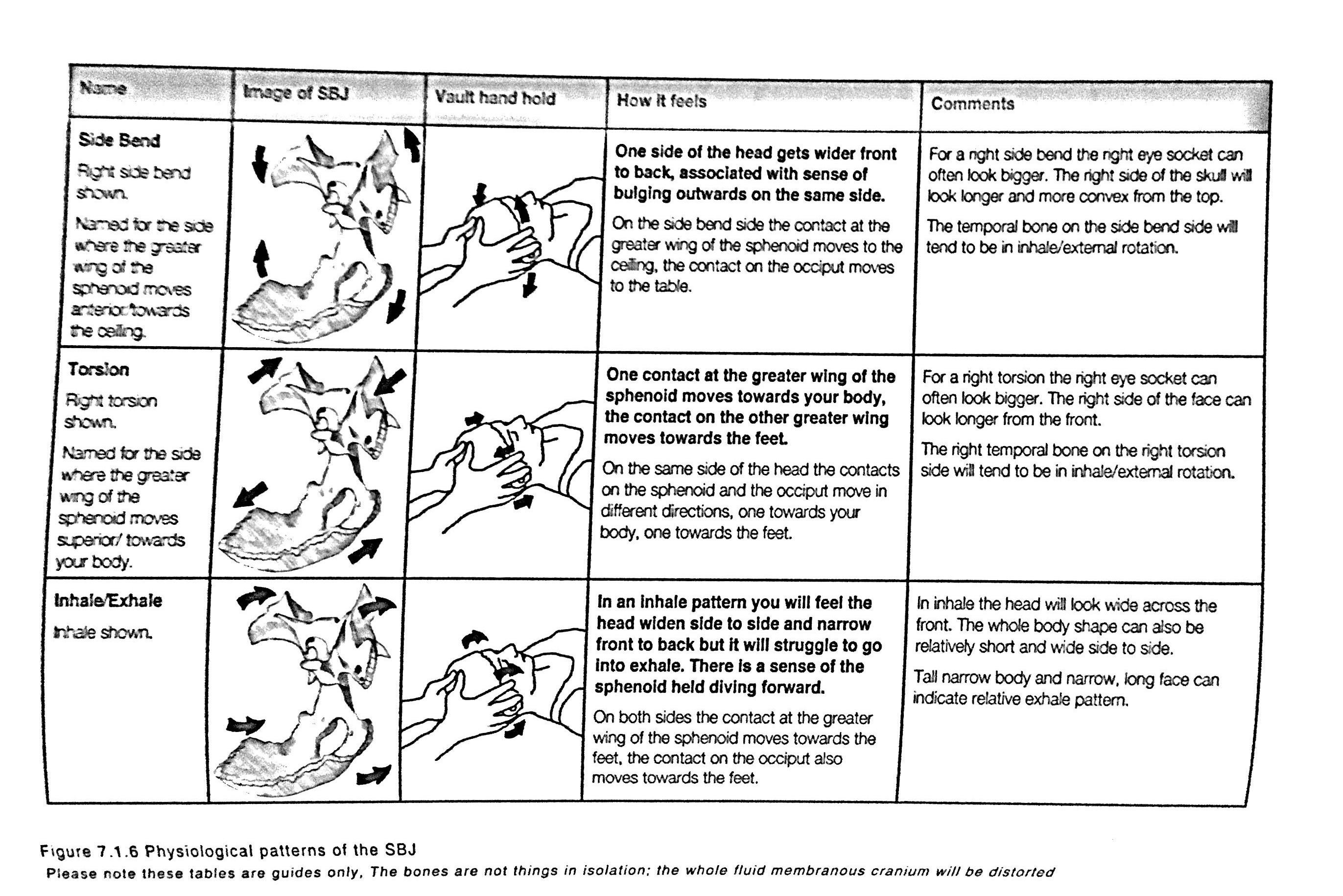
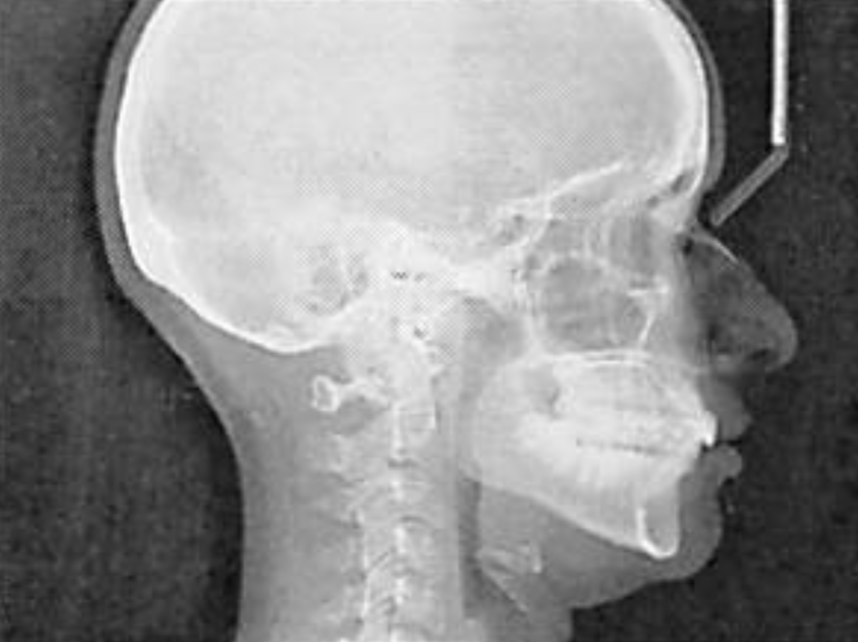
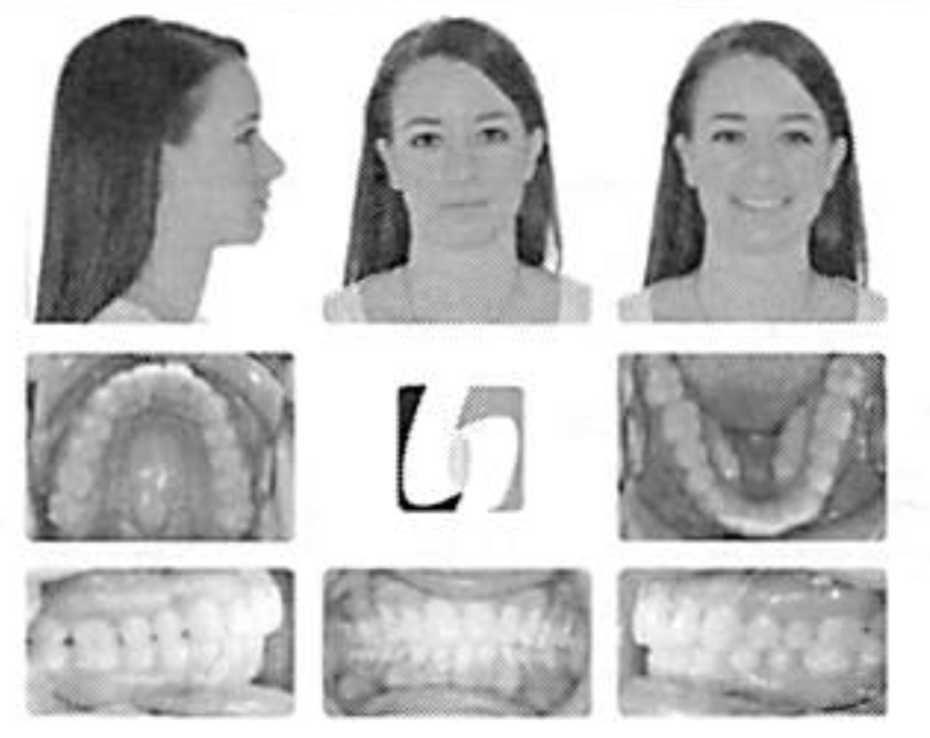
The following photo is a patient of an integrative dentist that works with a PRI physical therapist. The women shown is demonstrating a Right Torsion pattern, a narrow mandible, and a long narrow extended cranium. She had a tight chest wall, a lot of tongue activity, hyoid dysfunction, an overly straightened spine, a reversed cervical curve, and a narrow airway.
This understanding of how local facial, neck, and jaw muscles can malposition the cranium is generally understood. What Dr. Rothbart did is take the understanding of common cranial bone strain patterns and examined the relationship between the alignment of other bony structures.
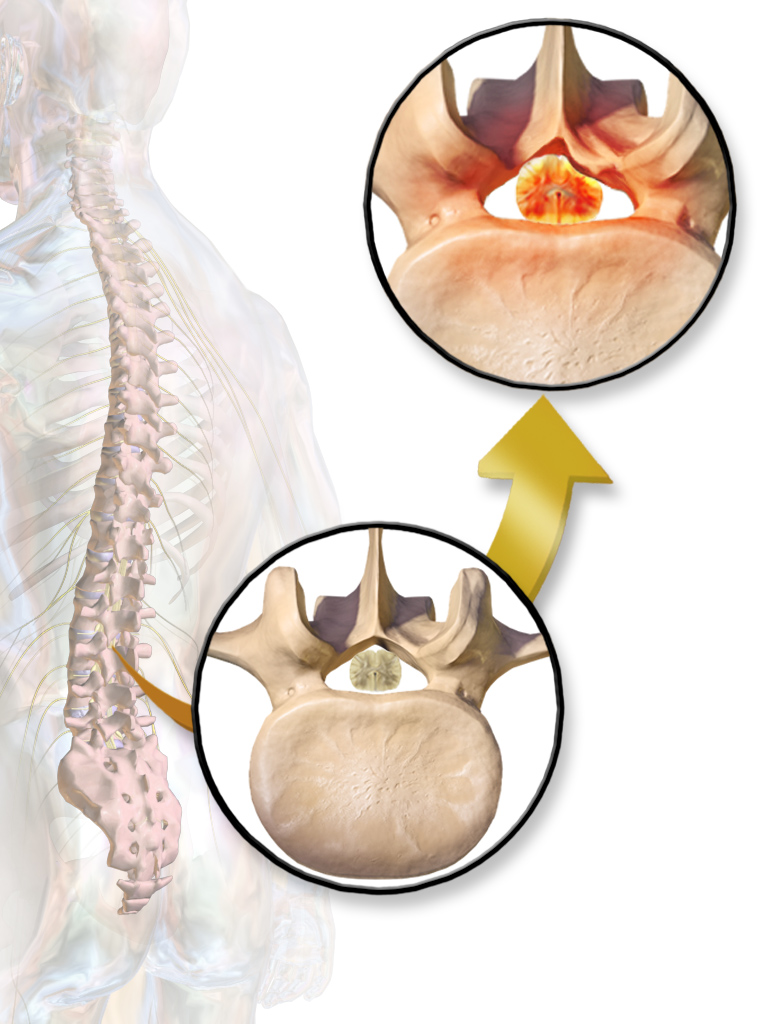
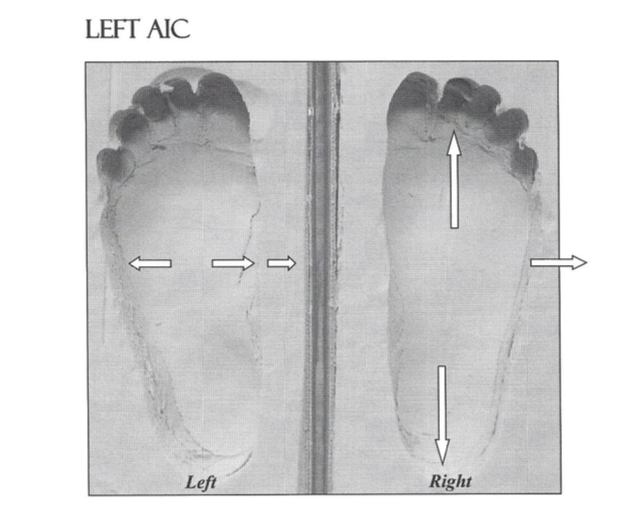
What Dr. Rothbart found in his study was that a dysfunction of the foot (pronation: a collapse of the arch of the foot) was associated with dysfunction of the pelvis and cranial bones.
Individuals with collapsed feet also had anterior pelvic tilt (low back instability) and anteriorly tilted temporal bones.
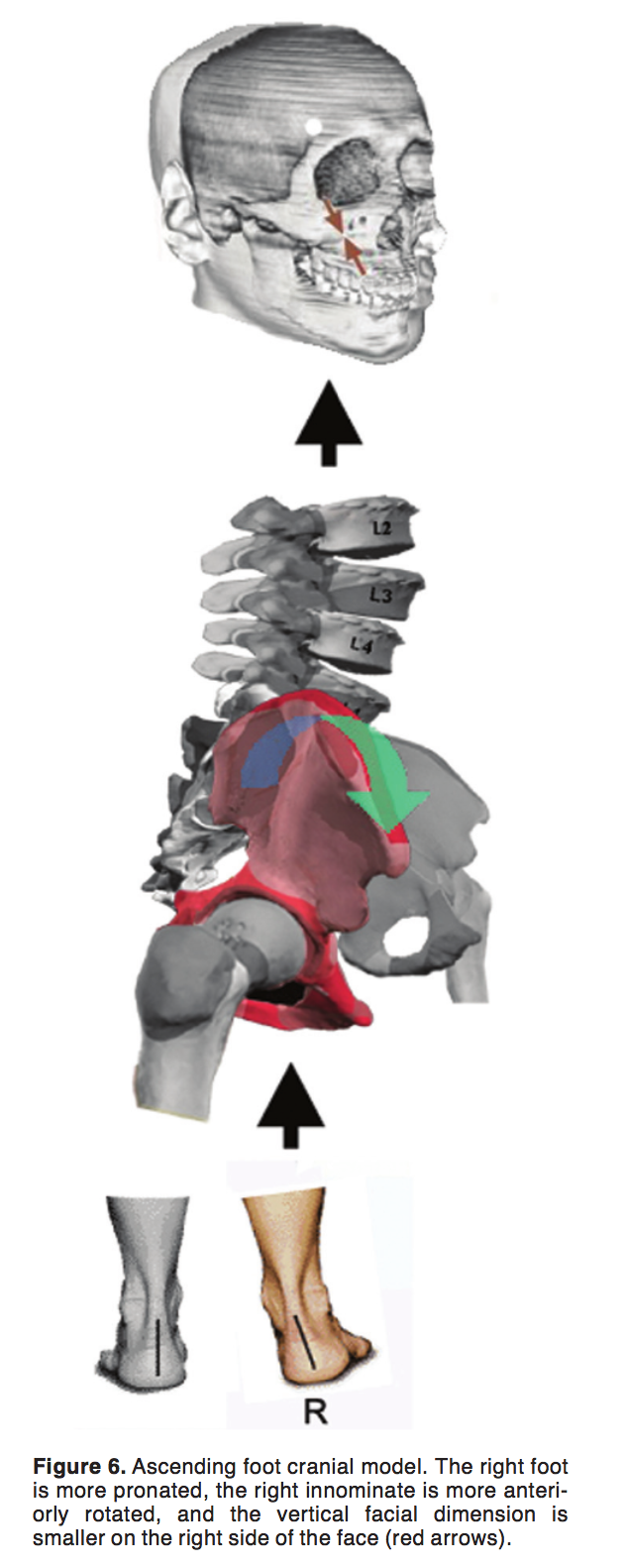
Pronation = Anterior Pelvic Tilt = Anterior Tilt of Temporal Bones = Loss of Vertical Facial Dimensions
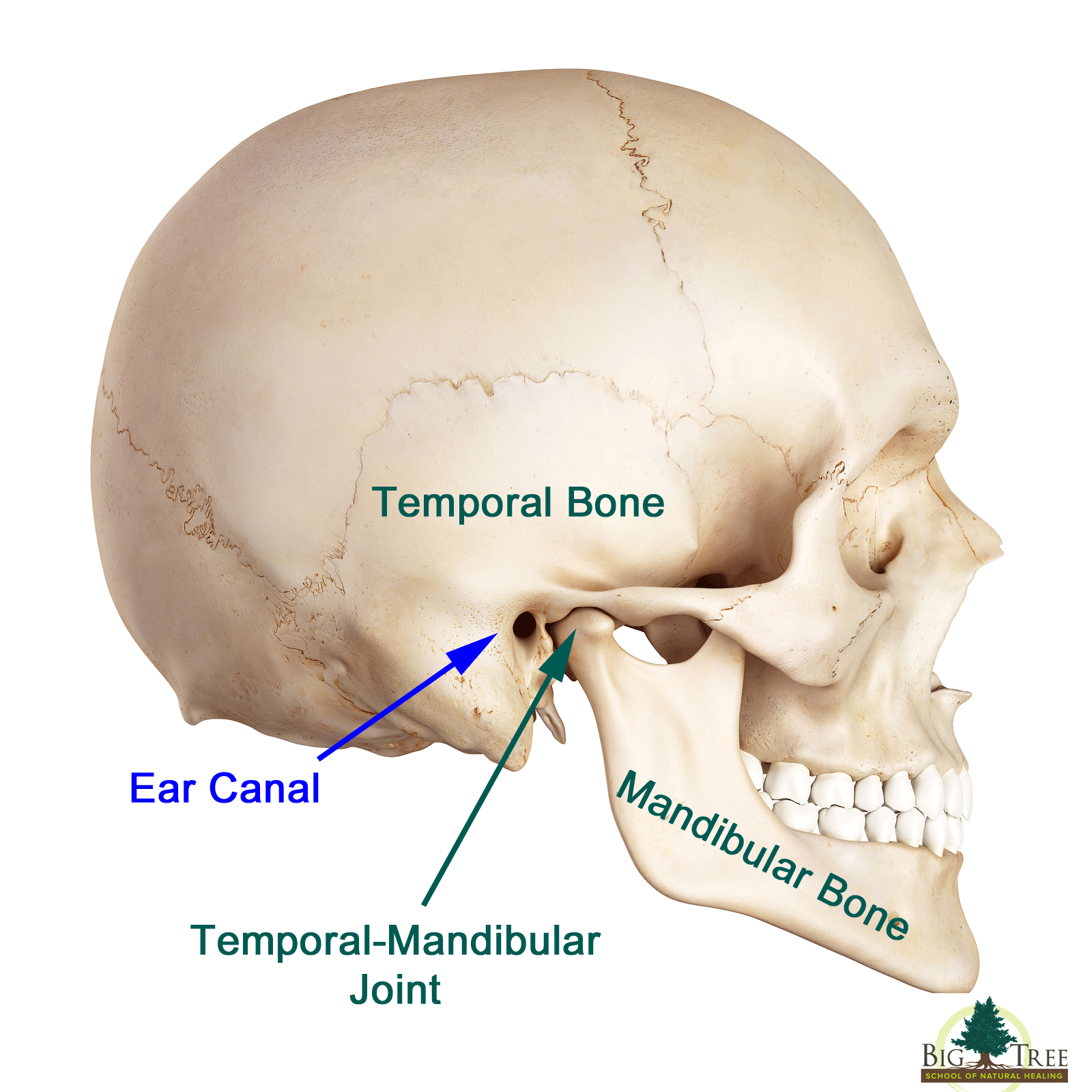
The image above shows how the position of the temporal bone will effect the TMJ.
Responses to Some Objections Before We Proceed…
Some practitioners reading this may object to discussions of predictable patterns. Structural Integrator (Tom Myers), for example, talks about different compensatory strategies that your soft-tissue may use to hold pronation of the foot or anterior tilt of the pelvis in place.
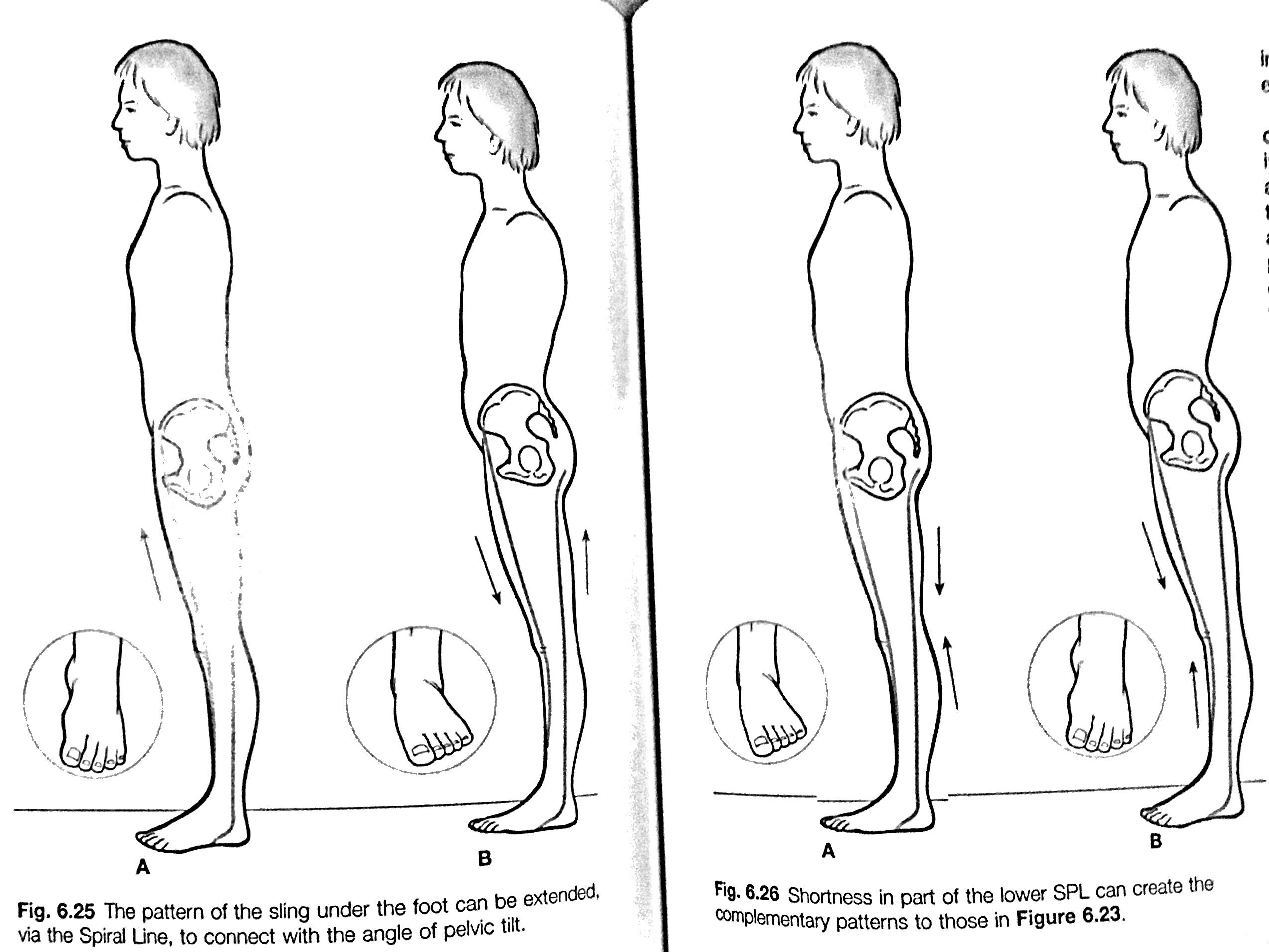
Tom here talks about how someone will compensate with a pattern of anterior pelvic tilt and a supinated foot. Another perspective is that of manual muscle testing where a common saying is used, “Assess Don’t Guess.” NKT (a type of muscle testing) practitioner Kathy Dooley talks about TMJ in her article, “Why You Use the Jaw for Motor Control.”
“Your TMJ is not the bad guy. He’s the compensating guy. Your overworked jaw is likely compensating for some missing components of motor control elsewhere in the kinetic chain. Get assessed and corrected as a movement system. The sum is always greater than its parts.” – Kathy Dooley
So, here (the brilliantly smart) Kathy is on the same page as Dr. Rothbart in suggesting that your skeletal alignment (posture/movement) will influence cranial bone positioning. Instability will commonly lead to tension in the jaw. She is simply asking us to assess why and how that dysfunctional pattern is being held in place.
http://www.drdooleynoted.com/anatomy-angel-why-you-use-jaw-for-motor-control/
I am a Level 3 NKT practitioner and have spent at least 150 hours in study groups learning muscle testing and how local restrictions (like a tight jaw) are related to global patterns. I am still learning.
HOWEVER, I have also run tests on hundreds of patients that look at the relationships that the Postural Restoration Institute and Dr. Rothbart have put forth. Certain relationships of bones certainly can be held in place by different muscle groups and stabilizing strategies but it can be very rewarding to keep an eye open to predictable patterns and pathological expressions of those patterns.
What I have found is that (women in particular that have TMJ) have excessive anterior pelvic tilt and LAX hamstrings. The hamstrings are the REINS on the pelvis and prevent anterior pelvic tilt. When they become overstretched or neurologically inhibited pelvic instability ensues.
#2: Why Would I Look for a Correlation Between Hamstring Laxity & TMJ?
The founder of the Postural Restoration Institute (Ron Hruska) made a very interesting statement at his Cervical Revolution course,
“When You Lose Your Connection to the Ground (Via Your Heels) Your Teeth Become Your Feet.”
Say What???
From a neurological and sensory perspective – someone who suffers from instability will resort to using another reference center to gain stability. This goes back to what Kathy Dooley was talking about.
To simply things (before delving deeper) here is the big takeaway.
Sensory input from the feet plays an important role in providing pelvic stability. The ability to sense the floor is dependent on neurologically engaged hamstrings (via sensory input from the heels) to prevent anterior pelvic tilt and instability that results in compensation elsewhere.
The 90-90 Hip Lift exercise grounds an individual through their heels (hamstrings) and facilitates abdominal integration via an exhale. This takes them out of an overextended hyperlordotic pattern where they over utilize their hip flexors and back extensors for stability. The heels are a reference center for the hamstrings.

In women with instability aka: overstretched hamstrings – that new reference center is oftentimes the teeth. Instead of being able to sense the floor for stability this individual will use the teeth to create a floor. Clenching ensues and overtime jaw pain (TMJ disorder) manifests.
Here is an example of the connection between the jaw and muscle tonus…
The dental appliance used in this video took away the teeth (occlusion) as a reference center which forced him to have to find the floor with his heels. This eliminated protective tension from the hip flexors and improved his straight leg raise.
An exercise you can try yourself is to contact your molars in the back of your mouth during a single leg balance exercise – notice how this affects your balance.
Some individuals may need their physical therapist to work with a dentist to expand the palate and create other changes. That is outside the scope of this article, the good news is that many individuals simply need to retrain their movement patterns.
Reference Centers – New Points of Stability
Someone that is always standing on their right leg oftentimes cannot efficiently load bear weight onto their left leg. They are lacking a left heel as a reference center.
The same person that has a pelvic orientation to the right and favors their right side is commonly pronated (collapsed) in their left foot and supinated (high arch) in their right foot. The reference center that will help them shift back to their left is their right arch. They need to sense their left heel to load on the left and sense their right inner arch to push off (pronate) on their right.
Finding and feeling (sensing) areas of our body is what creates changes in movement patterns – not just stretching and strengthening. Someone that is pronated on both sides (as in the Rothbart article) will resort to using secondary stabilizers and their jaw for stability. Note how in the video above the man was over-recruiting his hip flexors to propel him forwards until he was able to find the floor with his heels.
It is interesting to also note the relationship between ribcage flare and pronation. PRI Instructor James Anderson discussed this relationship at PRI’s Advanced Integration course. The asymmetrical nature of the right diaphragm tends to create left ribcage flair which in turn drives over pronation on the left foot. Overtime individuals will often exhibit bilateral ribcage flair (still more on the left) and bilateral pronation.
Look at the following picture of this young gymnast and ask yourself – where is she living in her body? You can see her anterior pelvic tilt? Does she look grounded? Can you see the posterior tilt in her ribcage? Do you notice her forward head posture? Do you see the compression in her low back? Can you feel the strain in her overlengthened hamstrings? Can you sense the tension in her jaw?

This site is a great resource for young gymnasts: http://shiftmovementscience.com
#3: How I Screened for a Correlation of Hamstring Laxity and TMJ
After taking the PRI course Cervical Revolution I began not just testing for hamstring laxity and looking at cervical alignment but correlating it to jaw pain. I was already screening the length of everyone’s hamstrings using tests for anterior pelvic tilt and hamstring laxity. I already worked in a clinic that witnessed much more TMJ in women than in men. What I began to do (over a 6-month period) is ask every woman who had jaw pain if they could palm the floor. The classical physical therapy textbook written by Kendall and Kendall, “Muscles: Testing and Function” states that palming the floor is a sign of pathology.
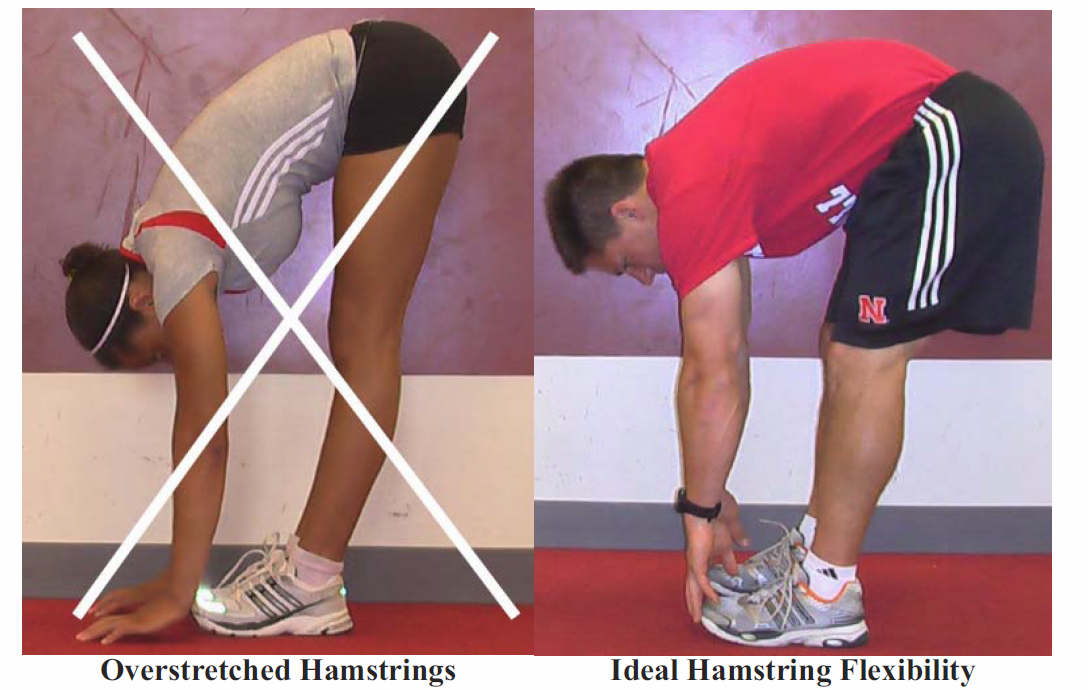
Someone that cannot fully achieve hip extension SHOULD NOT be able to palm the floor. Limited hip extension is an indication of anterior pelvic tilt – which SHOULD limit both the forward bend and the straight leg raise. Being able to palm the floor is an indication of pelvic instability. Having limited hip extension yet having a NON-restricted Straight Leg Raise is an indication of laxity. This is how I determined if they had hamstring laxity aka pathology.

I hope you can appreciate the danger in this situation – someone that has a lack of dynamic stability from the hamstrings has excessive anterior pelvic tilt, yet has the PERCEPTION of hamstring tightness.
There are two possible scenarios here:
#1: Someone with anterior pelvic tilt will have a NORMAL limitation in their forward bend and straight leg raise – this is appropriate protective tension
#2: Someone with anterior pelvic tilt will NOT have a limitation in these two tests – this is PATHOLOGICAL
It is in this second scenario that the jaw often becomes involved.
Scenario #1 over time leads to scenario #2 – excessive hamstring stretching leads to pathology. The person with a limited forward bend (in yoga) will further stretch their hamstrings to get into that position – even though IT IS NOT THE HAMSTRINGS FAULT!
The individual with a limited Straight Leg Raise will further stretch their hamstrings to improve the SLR – even though IT IS NOT THE HAMSTRINGS FAULT!
I call this, “THE VICIOUS CYCLE OF INSTABILITY”
I can bet that reading this right now you are clenching your JAW!

The Stretch to Win Institute talks about how Tom Myer’s anatomy train the Lateral Line can limit the SLR. Gray Cook (The Functional Movement Screen) has a nice saying, “The Straight Leg Raise is NOT a hamstring test.”
I did conduct additional tests to see how a woman who could palm the floor could stabilize her pelvis (Pelvic Ascension Drop Test/Muscle Testing), obtain neutrality of the hip (Adduction Drop Test/Muscle Testing), and shift into her left and right hip (Hruska Adduction Lift Test).
I did this to remain neutral in my observation process and because I worked with a lot of teenage female dancers who needed to have end range flexibility – that required greater hamstring length than most athletes.
The following study showed how hamstring and abdominal activation relieved IT Band tightness and restored hip extension (Obers Test):
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3563370/
#4: The Correlation I Found Between Hamstring Laxity and TMJ
What I found in a four-month period is that 12 women that had TMJ could palm the floor. I don’t have exact data as to how many women with TMJ couldn’t palm the floor. I wasn’t thinking of conducting a study – just casually noting the correlation.
This blog is meant to simply get you to factor in hamstring laxity with patients with jaw pain. It is an important factor that you should consider – it should not be overlooked. A lot of women with jaw pain that I have worked with also had low back pain. Many of these women were either doing yoga (hamstring stretching) and/or stretching because a physical therapist had prescribed hamstring stretching for their low back pain.
It wasn’t until I got them to stop stretching their hamstrings and hip flexors that their low back pain and jaw pain subsided.
One woman in particular who had struggled with consistent jaw pain for years reported absence of pain (for the first time in years) a few days after I prescribed her the 90-90 Hip Lift with a Balloon (which also repositions the sphenoid bone). I gave her this one exercise on her first visit to inhibit her low back and anterior neck muscles. Upon her second visit, she was amazed that after undergoing extensive physical therapy and regular chiropractic adjustments (with no improvement) that blowing up a balloon and activating her hamstrings could have such a profound effect globally.
Video of the 90-90 Hip Lift: https://www.youtube.com/watch?v=4GoqjoEXaAw
She asked me how I did it and I told her, “I didn’t do anything – you did it – you found the floor.”
I have also used this exercise with much success with patients with vertigo. One female patient of mine in her sixties had suffered from dizziness for years despite regular chiropractic adjustments. By working with her using the 90-90 hip lift, doing some manual therapy work, and a few other exercises she eliminated her vertigo and neck pain in just a few visits over the course of three weeks.
#5: Self-Treatment for TMJ Disorder
5A: Screening for Hamstring Laxity
The first question with TMJ is can you palm the floor? This is a strong indication of overstretching and/or neurologically inhibited hamstrings. Or as Ron Hruska puts it,
“Long, neuromuscularly weak, hypotonic, overly stretched (inactive) hamstring group.”
I have previously written about the need to exercise caution with the downward facing dog. I use the word caution because I would use orthopedic tests to determine whether or not such an exercise is appropriate for someone. Someone on their own (a woman doing yoga) can benefit from certain ‘rules of thumb’ like exercising caution in regard to over-lengthening the hamstrings.
5B: Core Stability for Hip Mobility
It is harder to assess your ability to achieve hip extension on your own but your ability to maintain a neutral spine in quadruped (bird-dog in yoga) is a good indicator of if you have the necessary stability prerequisite for hip mobility. Dancers, gymnastics and other athletes that require greater hamstring flexibility can coordinate these two tests.
The Prague School of Rehabilitation (DNS) has great exercises for developing high levels of stabilization in different positions. The hamstrings ARE NOT THE ONLY FACTOR in anterior pelvic tilt but an important one since APT strains the hamstrings. I have reset the pelvis with exercises that do not include hamstring activation. DNS talks about intra-abdominal pressure and the co-contraction of the diaphragm and the pelvic floor needed to balance the pelvis. I have even used tones (certain pitched sounds) with some individuals to reset the pelvis.
Check out this video of the BodMechanic working his magic (using tones):
https://www.instagram.com/p/BQmMjAwgRXy/?hl=en&taken-by=bodmechanic
Whether or not I decide to use hamstring activation depends on the interplay between tests. I most often do but that greatly depends on whether or not that they can palm the floor and how their symptoms manifest.
I spend A LOT of time on hamstrings with pregnant women – walking upstairs backwards, bridging, hip lifts, standing supported weight hamstring exercises, supplying multiple options in different positions.
Dancers and gymnastics that have spent years developing their body a certain way need to spent some time training end range positions for dynamic stability. I use Functional Range Conditioning to accomplish this.
Dr. Andreo Spina has a great Instagram page: https://www.instagram.com/drandreospina/?hl=en
From a manual therapy perspective, I use Fascial Stretch Therapy with individuals that require extreme flexibility. However, this does not involve passive static stretching – FST utilizes wavelike low grade PNF contractions at different ranges to neurologically develop control in that range. This is in line with Dr. Andreo’s statement that whether it be manual therapy or exercise – that stimulus is creating tissue changes accordingly.
5C: Airway Maintenance
Regular use of a netti pot greatly enhances airway health. Using filtered water and Himalayan sea salt clears the airway and prevents compensatory hyperactivity of neck muscles that contribute to a global pattern of lumbar hyperextension, forward head posture, and anterior pelvic tilt.
Alternate nostril breathing, chewing on both sides of the mouth, blowing up balloons, wind instruments, positioning breathing drills, sleeping with a cervical supportive pillow, and diffusion of essential oils are all useful practices.
5D: Walking Barefoot
While orthotics (when appropriate) and supportive shoes have their place, it is essential to spend some time each day walking barefoot. Probiotics, Vitamin D, and shoes are all conveniences that prevent us from actually choosing what’s best for us (eating fermented foods, getting sunlight, and grounding ourselves).
In fact, studies show that grounding (spending time outside barefoot on the earth) grounding improves blood viscosity, heart rate variability, inflammation, cortisol dynamics, sleep, autonomic nervous system (ANS) balance, and reduces effects of stress.
What better way to alleviate stress and jaw tension than to re-connect to the earth and to our own bodies?
Dr. Mercola does a nice job talking about grounding (earthing):
“Your immune system functions optimally when your body has an adequate supply of electrons, which are easily and naturally obtained by barefoot contact with the Earth. Research indicates that electrons from the Earth have antioxidant effects that can protect your body from inflammation and its many well-documented health consequences. For most of our evolutionary history, humans have had continuous contact with the Earth. It is only recently that substances such as asphalt, wood, rugs, and plastics have separated us from this contact.”
https://articles.mercola.com/sites/articles/archive/2012/11/04/why-does-walking-barefoot-on-the-earth-make-you-feel-better.aspx
Additional Resources on Grounding
Chevalier G, Sinatra S, et al. Earthing (grounding) the human body reduces blood viscosity—a major factor in cardiovascular disease. J Altern Complement Med. 2013 Feb; 19(2): 102–110.
Chevalier G, Sinatra S. Emotional stress, heart rate variability, grounding, and improved autonomic tone: clinical applications. Integrative Medicine. June/July 2011; 10(3).
Chevalier G, Sinatra S, et al. Earthing: health implications of reconnecting the human body to the Earth’s surface electrons. J Environ Public Health. 2012;2012:291541.
Chevalier G, Mori K, Oschman JL. The effect of earthing (grounding) on human physiology. Eur Biol Bioelectromagn 2007;1:600–621.
Chevalier G. Changes in pulse rate, respiratory rate, blood oxygenation, perfusion index, skin conductance and their variability induced during and after grounding human subjects for forty minutes. J Altern Complement Med. 2010;16:81–87.
Ober AC. Grounding the human body to earth reduces chronic inflammation and related chronic pain. ESD Journal 2003;July Issue. Online document at: www.esdjournal.com/ articles/cober/earth.htm Accessed March 17, 2011.
Ober AC. Grounding the human body to neutralize bioelectrical stress from static electricity and EMFs. ESD Journal 2000;January Issue. Online document at: www.esdjournal .com/articles/cober/ground.htm Accessed March 17, 2011.
Ober AC, Coghill RW. Does grounding the human body to earth reduce chronic inflammation and related chronic pain? [presentation]. European Bioelectromagnetics Association Annual Meeting, Budapest, Hungary, November 12, 2003.
– Kevin J Kula, “The Flexibility Coach”
Leave A Reply (No comments so far)
You must be logged in to post a comment.
No comments yet